Panicos Shangaris WebSite
 |
|
 |
![]()
|
Panicos Shangaris WebSite
|
|
|
™ A Major Neurological Condition ˜ EPILEPSY
Behavioural ScienceProject
Prepared By: Panicos Shangaris E-mail: shangaris@yahoo.com
“Do poor Tom some charity, whom the foul fiend vexes.” - William Shakespeare, “King Lear”, Act III, scene IV.
El Bosco (1460-1516)
Epileptic Girl (1510)
A Major Neurological ConditionEpilepsy
1.1 Generally: The word epilepsy is derived from the Greek verb (epilamvanein) ("to be seized," "to be taken hold of" or "to be attacked"). In ancient Greece, as now, people spoke of "having seized" and of having had an "attack." This terminology derived from the even older notion that all diseases represented attacks by the gods or evil spirits, usually as punishment. Even in comparison with all the advances made during the last century—more than at any other time in history—consider how enormous and fundamental was that first step attributed to Hippocrates in about 400 bc: that epilepsy is a disease of the brain that must be treated by diet and drugs, not religious incantations. Epilepsy is, of course, not a specific disease, or even a single syndrome, but rather a broad category of symptom complexes arising from any number of disordered brain functions that themselves may be secondary to a variety of pathologic processes. The terms convulsive disorder, seizure disorder, and cerebral seizures are synonymous with epilepsy; they all refer to recurrent paroxysmal episodes of brain dysfunction manifested by stereotyped alterations in behaviour. Today, a large number of clinical phenomena are recognized as epileptic seizures, some of which (e.g., myo-clonic and atomic seizures) are currently poorly understood and might, in fact, reflect neuronal mechanisms that are somewhat different from the path physiologic processes traditionally considered to be "epileptic." A variety of conditions or epilepsies have been categorized and defined not only by the types of seizures they manifest but also by other, associated clinical features. Specific epileptic syndromes have been identified by their characteristic seizure types, pattern of seizure recurrence, age of onset, associated neurological and other clinical signs, electroencephalographic (EEG) findings, presence or absence of familial occurrence, and prognosis.
1.2 Classification: They are useful in helping us in the treatment and counsel of our patients and/or enable us to understand the basis for a patient’s epileptic seizures. Similar ictal behaviour changes can result from different substances in relation to treatment choice is not as clear as we like to believe. The limitations of seizure classification is that it describes common seizure phenomenology only.
Different types of epilepsies are shown below: Generalized Epilepsies: · Benign myoclonic in infants · Juvenile myoclonic epilepsy · Childhood absence epilepsy · Juvenile absence epilepsy · Epilepsy with generalized tonic clonic seizures in childhood · West’s syndrome (infantile Spasms) · Lennox Gastaut syndromes · Epilepsy with continuous spike and waves in slow wave sleep (ESES) · Landau Kleffner syndrome · Rasmussen’s syndrome · Epilepsy and inborn errors in metabolism
1.3 Aetiology: Epilepsy occurs when nerve cells in the brain fire electrical impulses at a rate of up to four times higher than normal. This causes a sort of electrical storm in the brain, known as a seizure. A pattern of repeated seizures is referred to as epilepsy. Basic research aims to identify viral, genetic, or other factors that cause epilepsy. These findings provide the basis for developing new and improved methods of prevention and therapy. Scientists are using promising new technologies such as positron emission tomography (PET) and magnetoencephalography to diagnose epilepsy and pinpoint seizure location.
1.4 Drug Treatment:
Medication controls seizures for the majority of patients, who are otherwise healthy and able to live full and productive lives. On the other hand, at least 200,000 Americans have seizures more than once a month. Their lives are devastated by frequent, uncontrollable seizures or associated disabilities. The goal of modern neurological research is to develop safe, well-tolerated drugs that control seizures. Basic research has brought some of the now more commonly prescribed anticonvulsant drugs to the market. Scientists are also developing ways to test new and better drugs in patients.
1.5 Surgical Treatment:
This form of treatment, performed at epilepsy clinical research centres, is now an option more available for people with epilepsy, including children. For patients whose seizures cannot be controlled with drugs, surgery can turn the dream of a seizure-free life into a reality. Improved technology has made it possible to identify more accurately where seizures originate in the brain and to what extent surgery may affect vital functions, such as smell and speech. 1.6 Other Types of Treatment: Neurostimulation and especially Vagus Nerve Stimulation (VNS). VNS is now an accepted therapeutic alternative for patients with difficult-to-treat seizures.
Fig. 1 Sagittal, spin-spin, magnetic resonance. An astrocytoma with refractory frontal lobe epilepsy.
1.7 Social Issues: Although considerable progress has been made relative to the social adjustment of people with epilepsy, there remains much to be done. Considerable challenges face those in less industrialized countries in which some of the issues in discrimination, employment, and so on, are only recently becoming obvious and receiving media attention. As discussed by Ceilings (1994), we are only at the beginning of examining international differences in psychosocial well being and quality of life for this population. The challenge remains to not only identify these differences, but marshal available funds in order to mount education and the other psychosocial intervention efforts that currently are lacking.
1.8 Psychiatry and residential care:
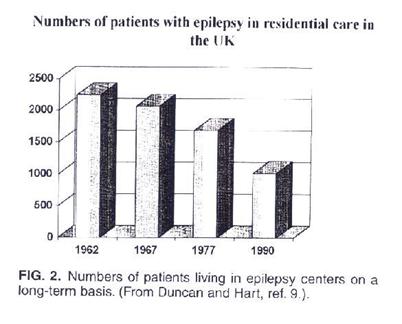
On the site of the traditional countryside residential setting, services are being developed to provide residential assessment away from the clinical atmosphere of the hospital. Epileptic patients with challenging behavioural and learning disabilities can undergo specialized assessment and treatment in this setting. A special role in the future might be found for work in the field of forensic neuropsychiatry. Certainly the trend to shorter, focused admissions will continue, with the centre at the same time reaching out to the community and offering preadmission services and post-admission follow-up. Some epilepsy centres in Europe are actively developing provisions for care in community projects by establishing small living units that are closer to patients, friends and families. Although residential schools are taking on the function of short-term assessment and rehabilitation, it is likely that at least some children with complex epilepsy and associated neuro- psychiatric problems will receive a large part of their education in such places. Epilepsy centres will continue to be involved in teaching and research. The question remains whether truly integrated services comprising health, social work, and education can continue to thrive in a social market. Only time will tell.
1.9 Social aspects, stigma, beliefs…
The following review yields some suggestions for ways clinicians can reduce the stigma attached to epilepsy. Patients are taught how to describe and manage their condition when they are first told about it. The clinical view is not imposed on the patient, but rather patients' beliefs fears about their condition and its diagnosis, treatment, and outcome, are explored. Epileptics can be marked by todays society due to their constant need for medication and medical care. Especially among children, medications are eliminated as soon as possible. Taking drugs may be a way to reduce conflicts with parents, and visits to the doctor may be prompted by a desire to keep a driving license rather than to take medication. A patient's family and social network have to be considered as an important source of support or discouragement for medical treatment as well as social and psychological adjustment. Patients have to be sent to other expert sources of assistance, vocational rehabilitation counsellors, psychological counsellors, self-help groups, family therapists, nursing staff and social workers.
1.10 Social and Psychological Problems:
If parents are overly protective and concerned about the possibility of a seizure, they may over restrict the child’s activities and hinder the development of life skills. For example, children with epilepsy have been found to be more parentally dependant than children with tonsillectomies.
Empirical research carried out to identified factors associated with social dysfunction in persons with epilepsy identifies the following as risk factors:
The ultimate goal of support services is to help people with epilepsy and their families become as socially capable and competent as possible. There are three general guidelines to consider when making decisions about which services to use:
Although many people with epilepsy function well socially, others experience myriad problems. Comprehensive assessments should be carried out on a regular basis to facilitate early identification of social problems and referral for rehabilitation services.
1.11 Conclusion:
There's still, commonly, the concern that epilepsy is contagious, that epilepsy necessarily means that someone will have brain damage, that epilepsy makes someone unfit to reproduce, to parent, which is not true." However, the potential of new investigative tools, especially those of brain imaging and molecular biology, are providing unparalleled and unimagined insights into the mechanisms of epilepsy and epilepsy-related brain dysfunction, and are offering greater hope than ever before for prevention, effective treatment, and even cure.
Word Count: 1492
2.1 Questionnaire for Medical Professionals On Epilepsy as a Major Neurological Condition1. Can you tell us what actually Epilepsy is? (i) Can it be considered as a disease, psychological problem, virus, mental disorder, or anything else you have in mind? (ii) Is it inherited? (iii) Are there a lot of types of Epilepsy? 2. Could you tell us something about epilepsy in ancient Greece? 3. Could you give us a rough idea of how common is in Cyprus?
4. Does Epilepsy occur in all the ages or is it specific to some?
5. How do patients respond to their diagnosis?
6. How do these kind of patients appear in their active lives? I mean physically, socially, mentally and psychologically.
7. What are the possible causes of Epilepsy?
8. Do you think patients experience problems with their work if not why?
9. Does Epilepsy influence the relationships of the patients with the people they are dealing or work with? If yes, what do you suggest they do about it?
10. Is there any specific treatment for dealing with these patients? If yes, what is this way of treatment?
11. What is the importance of family, friends, and relatives in the support of these patients? How can they help?
12. Are there any specific intensive care units at the hospital for treating epileptic people? (i) If yes: what's the hospital programme? (ii) If no: Should they have a program? How should the unit be organised (under what conditions?)
13. How do you think society treats these people? (i) Is there any kind of discrimination? (ii) Is our society well informed for Epilepsy?
14. What possible problems may develop in the families of those patients?
15. Are there any economic problems faced by epileptic people?
16. How would you personally treat an epileptic patient? (What do you suggest is best for the patient?)
Patron saints of epilepsy Saint Antonius
2.2 Questionnaire for Patients On Epilepsy as a Major Neurological Condition
2. When was the first seizure? What was your reaction when the doctor diagnosed the condition as “epilepsy”, your first thoughts?
3. What was the reaction of your family? Did they change their behaviour towards you? Did they begin to be over protective? Do you think that this over protectiveness had a negative effect on you?
4. How often do you have seizures and what is the reaction of the people close to you?
5. Do you think that your behaviour has changed; from the day you were diagnosed with this condition? If yes, how?
6. In the workplace (school) what is your colleagues (classmates) reaction to your condition.
7. Do you have any problems with your job or your performance, because of this condition?
8. What was the reaction of your superiors? Do they have different approach for you, rather for your colleagues, or they just ignore your condition?
9. Any problem sleeping, nightmares maybe?
10. Do you feel that your friends discriminate against you? (Negative or positive) Do you have any problems in making new friends?
11. Do you feel that you are stigmatised by your condition. That is all that people are thinking about when they see you?
12. Comment on the fact that in some countries like Russia and Japan, driving is prohibited, by law, for people with medical history in epilepsy. (Literature)
13. Do you know how epilepsy can be treated?
14. What kind of drugs do you take? Do they have any side effects? Do they affect your quality of life?
15. Do you think that your self-confidence and personality have been affected by this condition?
16. Have you met any people that reacted negatively to you because they know about your problem?
17. Do you feel uncomfortable talking about this? Do you try to hide it?
18. Do you think that the community and generally the people that are closest to you; can help you override this problem psychologically and see things from a positive angle?
The epileptic mind
3.1 SUMMARY OF THE INTERVIEW WITH DR. P.
Dr. P. is a Neurologist and works at the Cyprus Institute of Neurology and Genetics. He has the most of epilepsy cases in the institute. In his own words he explained to us that Epilepsy is a neurological condition that is characterized by recurrent and unprovoked seizures. Dr P. said that about 50% of the forms of epilepsy are inherited. The others are so called are acquired from trauma, infections and anything else that disturbs the integrity of the nervous system. Dr P. said that there are two main categories and they have several subdivisions. Epilepsy comes from the ancient ages, as Dr P. confirmed and he said that the oldest description of epilepsy is in Babylonia tabloid, is in the British museum. It was called a sacred disease in ancient Greece. The percentage of epileptic people in Cyprus is the same as world wide, it affects 1% of the population. So are six thousand to seven thousand epileptics in Cyprus. The age ranges that are affected by epilepsy are mainly the young people, children and adolescence, even though epilepsy can occur in any age. Epilepsy is still stigmatised in Cyprus as well as in many other parts of the world, Dr P. said. In families with a history, it’s more readily accepted. People react badly; sometimes they deny their condition, that’s why sometimes they have problems, initially when they begin treatment. Also we can see the denial from the parent’s side, as they don’t want their child to take drugs. He said that most of the epileptic patients (approximately 70%) respond readily to their medication and have no further seizures. If they fall in to the other 30%, they so called resistant epilepsies, where treatment does not help them, obviously their whole life is affected, they can not work, they can not have a social life, they have restricted activities but obviously interferes with their quality of life. The causes of epilepsy are mainly genetic, many genes have been identified as the causes of epilepsy, and they are the so called acquired. Trauma is another cause, especially in Cyprus, because of the very bad driving of the Cypriots. Thus there is a huge amount of post-traumatic occurrences. The patients don’t experience problems with their work if their seizures are controlled. Dr. P. said that if they have side effects, from their medications, or their seizures aren’t controlled, sometimes they are stigmatised, they loose their opportunity to rise in their work, to get promoted etc. In their social life they can’t find wife or husband. He also said that epilepsy, would effect the way people deal with this family members especially if they have a paroxysm disorder, like epilepsy paroxysm. The treatment for epilepsy is basically several classes of anti-epileptic medications, different ones work better for different forms of epilepsy. There is also a special diet, called the ketogenic diet. It works better with children with catastrophic types of epilepsies; these are very severe forms of epilepsy that do not respond to any other treatment. There are also some devices, implants that can be used, something called the vagonerve stimulator. This is a device, which stimulates the vagal nerve, like a pacemaker, it sends inhibitory impulses up higher in the brain and controls seizures to some extent as a last resource there is surgery for certain forms of epilepsy. Dr P. said that if the epileptics are children they need the support of their parents to take their medication and be protected from potentially harmful activities, like climbing up trees, they might have a seizure and they might hurt themselves. Adults, and children need the psychological support of a family, their acceptance, not rejection, so they can deal with their illness more effectively. Sometimes this becomes difficult, sometimes the patients need to see professionals, psychiatrists, for family as well as individual therapy. He also talked about the care unit for epilepsy in Cyprus, which is one neuro-surgical intensive care unit in the Nicosia General Hospital that admits people with so called status epilepticals, which is a form of a seizure, which is prolonged, lasts more than 30 minutes, or repeated seizures without the person regaining conciseness in between. He also said that there are plans to set up here an epilepsy monitoring unit, using video EEG technology to record seizures as well as the clinical manifestations, for pre-surgical evaluations. Dr P. pointed out the lack of understanding and discrimination, and said that is important for people with epilepsy to form organizations and support groups so as to gain some form of influence, to demand their own rights. Our society could be better informed about epilepsy he said. A lot of people don’t know what epilepsy is, or they confuse it with satanic position, witchcraft. Other people confuse it with psychiatric diseases even though there are psychiatric manifestations in epilepsy is an organic disease of the brain. The other problem that arises from epilepsy is a loss of income because the patient may not be able to work. He or she may not be able to take care of his or her children effectively, so income is usually affected unless the epilepsy is well controlled. But there are also children, sisters of a patient; brothers may not be able to find spouses because of the stigma association. The treatment that Dr P. takes for each patient is individual and he said that it depends on the kind of epilepsy, their age, and their situation. Some people need drugs, some people need a special diet, some people need modifications in their lifestyles, and some people at the same time need to see a psychologist. The main treatment though, is using anti-epileptic medications.
Epilepsy Surgery (Tlazolteotl)
3.2 SUMMARY OF THE INTERVIEW WITHDR. K.
Dr. K. is also a neurologist at the Cyprus Institute of Neurology and Genetics and he gave a more scientific approach on epilepsy and he said that it encompasses a number of syndromes. It may occur because of a disorder, due to the spontaneous discharge of a group of neurons in the brain, which give rise to a variety of clinical manifestations according to which populations of neurons are involved, e.g. if the neurons in the temporal lobe are involved the patient may experience a variety of autonomic symptoms, olfactory hallucinations, visual hallucinations with virtual alterations at the level of consciousness. Alternatively if the discharging neurons are in the diencephalons, generalized seizures occur with those at the level of consciousness and tonic clonic convulsions. Dr K. said that, epilepsy could be inherited. His answer for the question on the ancient origin of epilepsy said that it was recorded in ancient Greece and one of the treatments was to let the patient live alone to live the spirits get out. Dr. K. seemed that epilepsy could be found at all ages. There is epilepsy in childhood and at the old age, the aetiology of course is different at different ages. He said that the patients initially accept epilepsy with denial and also worry about different things like if they are still going to be able to drive, if it is inherited etc. Epilepsy affects a person’s day to day life in proportion to the patient’s attitude. A percentage feel fear of rejection from the others and a percentage live an active and normal life. And of course it depends on how severe the epilepsy is. Dr K. said that the possible causes of epilepsy are genetically acquired, congenital malformation of the brain, cortical displasias. In genetic different types, like genetic myoclonic epilepsy acquired, the reason may be from trauma, infection, encepalopathy, meningitis, tumours, cerebrovascular disease etc. The patients do experience problems with their jobs because they feel fear of having a seizure at work, of the side effects of medication on their performance, and also psychological problems affecting their outlook on their job. He also said that this condition affects the relationships of the people surrounding the patient. People may not accept that those people are cable of doing their job properly. Dr K. said that psychological support has to be given to these patients. They have to be informed about epilepsy. Then you follow a drug therapy, according to the syndrome. Each drug is suitable for a particular syndrome. The psychological support provided by the patient’s family and relatives is extremely important. They have to accept the patient for what he or she is. Support him practical as well as psychological support; treat them as equals. He said that Cypriot society needs an epilepsy service on call with necessary facilities. There are no suitable units in Cyprus. There is a great improvement from the society’s view for this condition, but there is still discrimination against those people. He thinks that society is not well enough informed about it. A lot, of problems will be faced, by the epileptic patients, like: Financial implications, psychological problems, stigmatisation of the family by the society, interfere with social needs of the family. Dr. K. said that in order to give the right treatment to the patient, we must first make sure that the diagnosis is correct, identify which syndrome corresponds to the case, give psychological support and finally drug therapy.
Epilepsy motifs in sculptures “Your mind is your force”
3.3 SUMMARY OF THE INTERVIEW WITHDR. Z.
Dr. Z. is a psychologist at the Cyprus Institute of Genetics. She says that epilepsy is a disease of the central nervous system, of which the aetiology is organic. A high percentage of the disease is inherited and there are a lot of types of epilepsy. It can be caused by an accident, from a tumour, stroke, anything that can cause damage to the central nervous system, or an anatomic anomaly from birth. She also explained us the origin of the word epilepsy and she said that is an ancient Greek word. “Epi” and “lambanon”, which means that something is received by the brain, that something is happening in our head, and we can’t control it. Something is occupying our brain. It was considered to be a secret disease; they said that it was related with the full moon. It was considered as a secret because the patient looses his control and then totally regains it. Dr Z. said that only in the institute of Neurology and Genetics there are approximately one hundred to one hundred and fifty patients but she didn’t know now many exist outside the Institute. There are more cases during childhood, adolescence, of which the cause is usually genetic, and for older ages usually the aetiology is a tumour, or post – traumatic epilepsies. People, she said usually don’t accept epilepsy easily. This may be because it is a condition that needs continuous monitoring. A large percentage of epilepsy, during childhood is not just epilepsy, but a combination of syndromes and genetic aetiologies. So this influences the mentality and personality of the patients. There is something that is called the epileptic personality, which is not an easy personality. There are some types of personalities that are easier to handle. They can reach a level or education in some types of epilepsies; the post – traumatic epilepsies, in combination with other kinds of problems. So we have an impact on their quality of life. Dr Z. said that the causes of epilepsy during childhood are mostly genetic, during older ages: the structure of the brain, post – traumatic causes, tumours. She also said that most of the patients have problems at work. This is because of the personality change of the patient, the disease. Most of them are not allowed to drive, drink alcohol, have many side effects from the drugs they take; they are depressed and they are falling asleep. So the impact on their life is obvious. The treatments available are: the anti-epileptic drug therapy, and the surgical treatment, which cannot be applied to all patients. The surgical procedure is not done in Cyprus. She said that the family has to become informed about epilepsy. They have to ask for the support of a specialist, a psychologist, they can take family therapy. So they can be helped to deal psychologically with the problem. Dr Z. said that in the Cyprus Institute of Neurology and Genetics they have most of the epileptic patients in Cyprus. Unfortunately they don’t have any specialised centre for the epileptic patients. There is no surgical team that can operate on an epileptic patient; we are at the beginning. We just have simple encephalograms. She also thinks that in Cyprus, in a large extent there is no discrimination. She said that the idea of the “secret” disease has been override. If society is not informed, which Dr Z. thinks it is, the people surrounding the patient are capable of informing the society about the disease, and telling the people that is not something deadly or supernatural. She said that the most common problems, which these patients face, are: the loss of their job and financial problems. Also, the creation of a myth around the disease; especially among the children, if one of their parents has it. They will be afraid of having seizures themselves. Dr Z. said that in order to treat the syndrome you have to find the aetiology. According to the syndrome there are a lot of types of drugs. If the patient does not respond to the drug she would change the drug. If nothing happens with the drug therapy she can proceed to the surgical solution of the problem.
Alt-Otting, Bavaria
3.4 SUMMARY OF THE INTERVIEW WITH Miss (X)
When I was told that my first interview, given to me by the Institute of Neurology and Genetics, was with a girl just fourteen years old, I was afraid. I said to myself, how am I going to deal with this patient, she is so young for an interview. When I met her I completely changed my mind. She seemed very understanding and mature. When I asked her about her condition, she tried to explain to me what it is but she couldn’t say it with scientific words. She explained it to me with her own words, what happens when a seizure comes. She said that she feels nothing, she just feels her hand moving and that her mother says that she has her mouth open during a seizure. This, she said, lasts for one and a half minutes. She said that the first seizure was six years ago. She remembered that because she had to spend her Easter vacation in the hospital. She said that she took it patiently. Her family started to react over protectively, even thought she didn’t say that clearly. She said that she used to have seizures very often, but now the seizures became very rare, probably due to the drug treatment. She must be a very mature girl because she said that her behaviour didn’t change, from the time she knew that she had epilepsy. Her friends know about her condition because of a seizure she had while she was on a school bus. Her friends treated her in the best way. Her performance at school she said, stayed unaffected. Her schoolteachers, while they know about the condition don’t show anything more than for the other students. . This is probably because they try to avoid any kind of discrimination. All her friends remained the same and she has no problem in making new friends. Because of her age, she doesn’t recognise the discrimination that society might have on patients with epilepsy, or she might just ignore the fact that this discrimination exists. On the question for the driving licence, she answered that epilepsy people don’t have any problems in driving, even thought she doesn’t drive. She was informed about the treatment of epilepsy, about drug therapy as well as for surgery and also informed that there are no units in Cyprus that can perform such an operation. She also knew the dangers on having this operation, for example the danger of staying handicapped. There are no side effects with her medication, and there is no impact on her quality of life. Her personality and self – confidence remained the same. She thinks that the society can help her to override psychologically her problem by having a positive altitude to her and convince her that this is just nothing.
3.5 SUMMARY OF THE INTERVIEW WITH Mr (Y)
Mr Y is a thirty -three year old, friendly man. He was a driver for a company in Cyprus. He used to carry cargos from one town to the other. When I met him he seemed very friendly with me and he tried to answer to all my questions. He said that he has this condition because of a car accident. When he has a seizure his mind stops, he is on another plane. The drug treatment helps him with his problem and now he knows when he is going to have a seizure and he sits and waits for it to happen. He had his first seizure approximately ten years ago. His first thoughts were about his family and his wife. He had a lot of help from his wife. He didn’t believe that the problem was such a serious one. His wife helped him psychologically and she convinced him to visit the doctor, she became over – protective and had a positive influence on him. He has a seizure two or three time per month. Many of his friends know about the problem and they are taking a good care of him any time he has a seizure. Epilepsy made him change the way he thinks and sees the world. He feels useless in the society, especially after he gave up his job. He feels a shame of himself. Here is may be the place where a good psychological support would be very helpful. He said that before he gave up his job his superiors and colleagues didn’t know about the condition. But unfortunately because of the kind of job he used to do, he couldn’t keep the condition a secret. There was a high risk of hitting other people from an unexpected seizure while driving the long car. So he gave up his job. He felt a strong friendship surrounding him, he found out his real friends. He noticed a kind of discrimination. He lives in a small village where everybody knows each other. So the problem cannot remain a secret. He agrees with the law, which prohibits driving for epileptic people, that’s why he gave up his job. You can’t endanger the people around. He seemed hopeless when I asked him about the treatment and he said that there is no real treatment. He said that the treatment just reduces the number of seizures. He said that the condition cannot completely, be treated. Even thought he said that his self –confidence has not been affected, I found that he was afraid to trust him self. He also said that people don’t trust him and they are afraid to ask something from him. He said that hiding his condition from the people depends from the people he is talking to. Society plays a great role on psychologically helping people with epilepsy. If someone doesn’t trust you because you have this condition, he forces you to be paranoid about the condition. This, according to him, increases the number of seizures dramatically. He gave me an example of his brother. His brother entrusted him with a dog farm and that reduced the number of seizures. He feels more comfortable with himself.
“Epilepsy Surgery” The stone cutter
3.6 SUMMARY OF THE INTERVIEW WITH Mr (Z)
Mr Z was a very nice thirty -one years old man. He works for a Brewery company in Cyprus and he was very happy talking about his condition. He got this condition as a post -traumatic damage in the brain, after a car accident, ten years ago. He had his first seizure six years after the car accident. He was well enough informed about the types of epilepsy, and he said that he did a kind of research through books trying to find information about his condition. He had very good support from his family. His only worry when he found out about his condition was his children. But his children, especially his first son seemed very mature and he is helping him any time he has a seizure. The family became over-protective and that had a very positive effect on his problem. He takes medication, and that he said reduces the number of seizures dramatically. His behaviour and personality remain the same. At work his colleagues and superiors are taking a good care of him. They are helping him psychologically and making him forget the condition and think something else. The problem after a seizure is that his muscles are tensed and he has to stay home for a week. But, because of the good relations with his boss, he faces no problem. The problem with his sleep is that sometimes he has insomnia, “it’s like something that warns you for a seizure” he says. He has no problem in making new friends and he has very good relations with his old friends. He doesn’t care what the people say about him, he said that he could handle his problem by himself and his friends. Here he seemed very self –confident, he knows the problem and he also knows the ways to overcome it. He agrees with the law, which takes away the driving licence for the epileptics, because of the danger of hitting someone by mistake. He knows that he will have the post- traumatic epilepsy for a lifetime, but he doesn’t seem to care. “The only thing you have to do, is to take your medicine,” he says. He hasn’t met any people that acted negatively to him and he doesn’t mind about talking about his problem. He thinks that the community can help epileptics by giving them a better job. Also, by organising a special program, for epileptics, inside hospitals. He also agrees that epileptic people need financial support.
Patron saints of epilepsy (Saint Cyriakus)
4.0 Conclusion
Having said all that and having interviewed each patient and each medical professional separately, we can extract a lot of useful information about the neurological condition known as epilepsy. The doctors helped me to understand all the difficulties the patients face practically and psychologically. Even thought there were some differences in between the three interviews with the doctors, we conclude that is not just the problem that matters. Society plays an important role for the treatment of such patients. We also found out that the society lacks a lot of facilities that are important for the treatment of those people. Each doctor basically follows a treatment according to the case and the patient. From each patient we extracted a lot of information and we have seen the way with which each patient has fought and still fighting epilepsy. The patients are trying to forget that they have any kind of problem and with the help of their own family and friend are able to do it. Two of the patients complained about the support given to them by the society, which is not enough for their problem. They are waiting for a more modern society, which has sent the man on the moon. From the interviews we see that the discrimination still exists but in a very small amount. Even though the discrimination is rare, the family of the patient cannot avoid labelling and stigmatisation, which still exist and make the life of those people difficult. So we hope that science will find new methods of treatment for this condition and that society will help these people with their psychological and any other problems they might face.
“What
doubtless remained longer than leprosy, and would persist when the
lazar houses had been empty for years, were the values and images
attached to the figure of the leper as well as the meaning of his
exclusion, the social importance of that insistent and fearful figure
which was not driven off without first being inscribed within a sacred
circle.”
Michel Foucault, Madness and Civilization: a history of Insanity in the age of Reason (11)
Saint Ubald of Gubbio German Epilepsy Museum
6.0 š References › 2. Van Laere KJ, Boon P, Vonck K, et al. Perfusion SPECT activation studies in acute and chronic vagus nerve stimulation. Program and Abstracts of the 54th Annual Meeting of American Epilepsy Society; December 1-6, 2000; Los Angeles, California. Abstract 100419. 3. Boon PAJM, D'Have M, Van Walleghem P, et al. Direct medical costs of refractory epilepsy incurred by three different treatment modalities, a prospective assessment. Program and Abstracts of the 54th Annual Meeting of American Epilepsy Society; December 1-6, 2000; Los Angeles, California. Abstract 100114. 4. Labar DR, Nikolov BG, Hosain SA, et al. Mood and anxiety changes in epilepsy patients treated with vagus nerve stimulation. Program and Abstracts of the 54th Annual Meeting of American Epilepsy Society; December 1-6, 2000; Los Angeles, California. Abstract 100249. 5. Hosain SA, Harden CL, Nikolov BG, et al. Vagus nerve stimulation in children with lennox-gastaut syndrome: a one-year outcome. Program and Abstracts of the 54th Annual Meeting of American Epilepsy Society; December 1-6, 2000; Los Angeles, California. Abstract 100704. 6. Epilepsy Syndromes A Guide (http://home.earthlink.net/~mchee1/episynd.html) 7. Epilepsy (http://www.medscape.com/LCM/InfMind/2001/03.01/) 8. Trimble MR, Dodson WE, eds. Epilepsy and quality of life. New York, New York: Raven Press Ltd., 1994. 9. Hauser WA, Hesdorffer DC. Epilepsy: frequency, causes and consequences. New York, New York: Demos Publications, 1990:1--52. 10. Begley CE, Famulari M, Annegers JF, et al. The cost of epilepsy in the United States: an estimate from population-based clinical and survey data. Epilepsia 2000;41:342--51. 11. Devinsky O, Penry JK. Quality of life in epilepsy: the clinician's view. Epilepsia 1993;34:S4--S7. 12. Collings JA. Psychosocial well-being and epilepsy: an empirical study. Epilepsia 1990;31:418--26. 13. Baker GA, Camfield C, Camfield P, et al. Commission on outcome measurement in epilepsy, 1994--1997: final report. Epilepsia 1998;39:213--31. 14. Buck D, Jacoby A, Baker GA, Graham JS, Chadwick DW. Patienl.s' experiences of and satisfaction with care for their epilepsy. Epilepsia 1996;37:841-849. 15. Achenbach TM. Manual for the Child Behavior Checklisl/4 Ifi. Burlington, VT: University of Vermont Department of Psychiatry, 1991. 16. Achtcrbcrg A, Nclcn W. The five-day epilepsy programme in Breda. Epilvpsichiilletin 1990:6. 17. Aldenkanip AP, Bijvoet MR. lleiscn TWM, SuurmeyerTPBM. The influence olepilepsy in parents on psychosoeial I'unclioning ol their children. Advtiiicvs in Kf)ilrfiti)liy\: Viil 17. New York: Raven Press, 19X9. 18. Arntson P, Droge I), Norton R. Murray \:. The perceived p.sycliosociiil consequences of having epilepsy. In: Whitman S, Hermann HP, eds. I'sychH/HilliiiliiKV in K/iili'/isy Nixw/ Dimrnxiiinx. New York: Oxford University Press. 19. Epilepsy and Art: Votive tables, paintings, sculptures. German Epilepsy Museum http://www.epilepsiemuseum.de/.
Jesus Christ as a healer of epilepsy
Special Thanks to
The End
Epilepsy motifs in sculpture Father and his epileptic son
|