Panicos Shangaris WebSite
 |
|
 |
![]()
|
Panicos Shangaris WebSite
|
|
|
Discuss screening methods of cancer of the genital tract of the female
By Panicos Shangaris, Dec 2003
1. Introduction Screening test is a test carried out on a large number of apparently healthy people to separate those who probably have a specified disease from those who do not. Limitations depend on the severity and frequency distribution of the disease and the efficiency and availability of treatment. Other factors to be taken into account are safety, convenience, cost, and sensitivity of the test [1]. Every 64 minutes, a woman in the United States is diagnosed with a gynaecological cancer. It is the fourth most common cancer in American women today. More than 82,000 [2] women are diagnosed each year with gynaecologic malignancies. Cancer diagnosed early can be treated quite well with much less discomfort with lifestyle changes and the use of available screening techniques. Gynaecologic cancer is an uncontrolled growth and spread of abnormal cells specific to the female reproductive organs, including the cervix, ovaries, uterus, fallopian tubes, vagina and vulva. Biomedical research has discovered that some genes, called oncogenes, promote the growth of cancer. You can acquire these genetic mutations during life (e.g. through smoking, aging or environmental influences) or you can inherit these mutations from your parents or grandparents. [3]
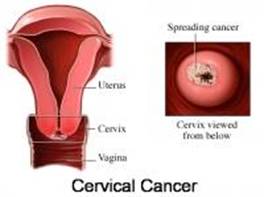
2. Cervical cancer
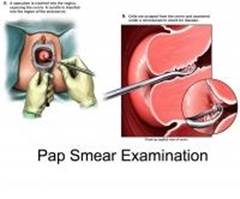
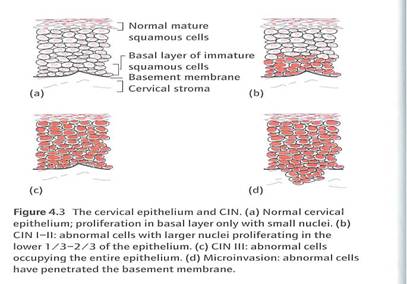
Globally, cervical cancer continues to be the second most common form of malignancy in women. It is also the leading cause of death from malignancy in developing countries. Generally the highest recorded rates in the world are in sub-Saharan Africa as well as in Central and South America and some regions of Southeast Asia. Cervical cancer has been one of the most studied of all human malignancies. In spite of this widespread knowledge regarding the epidemiology of cervical neoplasia, effective strategies employing this knowledge to impact on primary prevention have not been developed in any country to date. Most progress with regard to cervical cancer control has occurred due to cervical cytology screening programs [3]. The main screening test for cervical cancer is the Papanicolaou (Pap) smear. Although it sometimes detects endometrial, vaginal, and other cancers, its use as a screening test is intended for the early detection of cervical dysplasia and cancer. It is a non-invasive and inexpensive screening test for cervical precancerous disease that is easily performed in the office setting. Regular Pap tests should be performed on all women who are or have been sexually active and have a cervix. Testing should begin at the age when a woman first engages in sexual intercourse. Adolescents whose sexual history is thought to be unreliable should be presumed to be sexually active at 18 years old. There is little evidence to recommend an annual screening over three-year screening. Pap tests should be conducted at least every three years. The interval for each patient should be recommended by the patient's physician based on risk factors (eg, early onset of sexual intercourse, history of multiple sexual partners, low socioeconomic status). Women with human immunodeficiency virus should be screened more frequently. There is insufficient evidence to recommend for or against an upper age limit for Pap testing. Regular screening may be discontinued after age 65 in women who have had regular normal previous screening. Pap testing is not recommended for women who have undergone a hysterectomy in which the cervix was removed, unless the hysterectomy was performed due to cervical cancer or its precursors. Patients at increased risk of cervical cancer because of unprotected sexual activity with multiple sexual partners should receive appropriate counseling about sexual practices. Specimens should be sent to laboratories that have adequate quality control measures in order to ensure optimal accuracy. A thorough follow-up of test results should be ensured, including repeat testing and referral for colposcopy. Clinicians should provide patients with a pamphlet or other written information on the meaning of abnormal smears to help ensure follow-up and minimize anxiety over false-positive results. There is insufficient evidence to recommend for or against routine cervicography or colposcopy screening for cervical cancer in asymptomatic women or for those with human papilloma virus infections [4]. The Pap smear involves scraping cells from the external os of the cervix with a blunt spatula to gain cells from the transformational zone. It is also important to sample the endocervical canal. The sample is then placed directly on a slide or into a liquid based medium that is then used to make a slide. The prepared slide is examined by a cytopathologist [5]. Patients with abnormal smears showing dysplasia, squamous intraepithelial neoplasia, or two consecutive findings of atypical squamous cells of undetermined significance should undergo colposcopy and endometrial curettage. Neoplasia is categorized as invasive carcinoma or cervical intraepithelial neoplasia CIN [6]. (see table 1a&1b)
3. Endometrial cancer
Cancer of the endometrium, or corpus cancer as it was commonly called in the past, is a common form of pelvic malignancy in women and is most frequent in postmenopausal women. Considerable progress has been made in separating and classifying the various histological forms of so-called uterine cancers and better understanding their aetiology, treatment and prognosis. Primary uterine cancer is now generally well classified and separated into cancers of the cervix, uterine body, usually most commonly endometrial cancers, and also the less common but distinctive uterine sarcomas. Today we have a good understanding of the epidemiology and etiology of endometrial cancer [3]. Patients with endometrial cancer have abnormal uterine bleeding most commonly, postmenopausal bleeding. Ten percent of patients may present with leukorrhea. Occasionally, patients with cervical stenosis will not present with bleeding, but may have a pyometra or hematometra. There is currently no good screening tool for asymptomatic patients. Pap smears are unreliable for diagnosing endometrial cancer, given that only 50% of patients with cancer have abnormal cells detected on Pap. However some women on unopposed oestrogen, obese postmenopausal women, women with late menopause, premenopausal women with anovulatory cycles, and women on tamoxifen , may benefit from screening. Screening may be performed by office endometrial biopsy, or with ultrasound to measure the thickness of the endometrial stripe complex. (endometrial cancers have not been reported in women with stripes less than 4mm thickness)[14]. If an adequate endometrial biopsy cannot be performed due to patient discomfort, cervical stenosis, or insufficient tissue sample, a hysteroscopy and D&C should be done to visualize and sample the endometrium. In addition to endometrial sampling, the initial work should also include a pap smear. A pelvic ultrasound should be performed to rule out fibroids, polyps, and endometrial hyperplasia. If bone pain is present a chest x-ray should also be performed. The staging for endometrial cancer is surgical. (see table 2.) It is based on abdominal exploration, peritoneal washings TAH-BSO, and selective pelvic/periaortic node sampling is used to determine the extent of spread. Grade is a key prognostic factor [15]. (see table 3)
4. Ovarian cancer
Ovarian cancer is an important gynaecological cancer, particularly in industrialized countries where it usually ranks fifth or sixth amongst the most frequent forms of cancer in women. While we have come to better understand the various histological subtypes of epithelial ovarian cancer, their frequency, distributions and behaviour, the most important thing to note about ovarian cancer is that this is often one of the most common causes of death from pelvic malignancy in women when one excludes colon and rectal cancers. To date progress in determining precursor lesions, screening tests, early warning signs, etc. for this malignancy have not been fruitful. This disease does not present with any consistent early warning signs or symptoms so that the vast majority of patients who are diagnosed, are diagnosed with stage III or IV disease. The aetiology for ovarian cancer remains obscure. An increased risk has also been suggested for women who have a late age at first birth, early menarche and late menopause with some protection afforded by higher parity. This has led to the concept of ‘incessant ovulation’. It is thought that repeated ovulations produce tears on the surface epithelium and that the ultimate repair and regeneration process may subject the cells to influences that ultimately lead to the incorporation of surface epithelium into the subsurface areas of the ovary with eventual transformation into malignant epithelium. Of importance is the fact that several studies have now indicated that oral contraceptive use is protective against ovarian cancer with the incidence being reduced by approximately 40% in continuous users and to an even greater extent in individuals who have been long term users of these medications. The widespread use of combined oral contraceptive medication has probably been the major determinant of the recent favourable decrease of ovarian cancer rates noted in some western countries[3]. Symptoms usually do not become obvious until the tumor compresses or invades adjacent structures, ascites develops, or metastases become clinically evident. As a result, two thirds of women with ovarian cancer have advanced disease when diagnosed. There is no cost effective screening available for this kind of cancer. While tranvaginal ultrasound is promising, the false positive rate is very high. CA-125 is a serum marker that is expressed in over 80% of non-mucinous ovarian cancers, and is elevated in patients with early ovarian cancer. However, many benign conditions such as pelvic inflammatory disease, endometriosis, benign ovarian cysts, infertility, hepatitis, cirrhosis, congestive heart failure and also renal failure have been associated with elevated CA-125 levels. Because of the high false-positive rate for both CA-125 determination and tranvaginal ultrasound, these tests are not recommend for routine screening. There is insufficient evidence to recommend for or against screening of asymptomatic women at increased risk of ovarian cancer. The National Institutes of Health Consensus Conference recommends that women with presumed hereditary cancer syndrome should have an annual pelvic examination, CA-125 measurements, and transvaginal ultrasound until childbearing is completed or at age 35, at which time prophylactic bilateral oophorectomy is recommended.
Evaluation and treatment:
5. Cancer of the vulva
Carcinoma of the vulva fortunately is the least common of all of the major gynaecological cancers affecting the lower genital tract. In the first half of this century most patients presented with advanced, neglected tumours, which produced considerable morbidity and high mortality for these unfortunate women. It wasn’t until the 1950s, through the efforts of the late Stanley Way and others that a more effective successful surgical approach to the management of this disease occurred. Since that time, with improved medical care and better diagnosis, most patients are discovered at a much earlier stage of disease so that the number of patients with large, fungating, necrotic tumours has become uncommon in developed countries [3]. Usually occurs after menopause. The vast majority (90%) is squamous cell carcinoma. Risk factors include diabetes, obesity, hypertension, vulvar dystrophies, and HPV 16/18 infection. May presene with vulvar pruritus, but early stages are often asymptomatic. On exam the gynaecologist has to look for erythematous or ulcerated vulvar lesion and / or a palpable vulvar mass. Biopsy is necessary for the diagnosis. Staging is surgical (see table 5) and is based on tumour size, invasiveness, nodal involvement and distal metastases. Treatment is with local excision and regional lymph node dissection. Radiation is to reduce tumour burden and for metastatic or recurrent diasease [17].
6. Cancer of the Vagina
Vaginal Cancer is extremely rare and most likely represents metastasis or direct extension from cervical cancer. The most common is squamous cell carcinoma 85%, adenocarcinoma 5%. In 1970 clear cell adenocarcinoma was found to be associated with in utero exposure of diethylstilbestrol. (DES) Though vaginal cancer has been reported in every decade of life, it is predominantly a disease of older women with about 70% of patients diagnosed after the age of 70. Two exceptions to this rule are sarcoma botryoides and vaginal endodermal sinus tumour. These rare tumours demonstrate a predilection for infants and children. Most patients are asymptomatic. The most common presenting symptoms are increasing vaginal discharge, bleeding and pruritus. Screening is done with pap smear and follow up colposcopy, and pathologic diagnosis is made with biopsy of suspicious lesions[18]. (see table 6 for staging)
7. Conclusions
In summary we can see that the progress we have made in gynaecological cancer has been considerable. Clearly the scientific basis of contemporary medicine has benefited the female oncology patient. Widespread enthusiasm for the use of endoscopic surgery, particularly in cervical and uterine cancers, has yet to be translated into improved survival outcomes but has the potential for better anatomic staging and leading to the most appropriate available therapy with lesser morbidity and better quality of life. Advances in medical imaging, particularly CT scans and MRI, have greatly improved the ability to identify the extent of the disease and help plan therapy. Identification of oncogenes/viruses and the development of specific therapies against their molecular effects all signify the threshold of a new era in cancer diagnosis and therapeutics. While these developments will provide breakthroughs that will help in the battle against cancer in the future, we must not become complacent in our efforts and must constantly strive to develop solutions for those unfortunate women who do not have ready access to good standard medical care because of cultural or economic factors.
The End
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||